
Description:
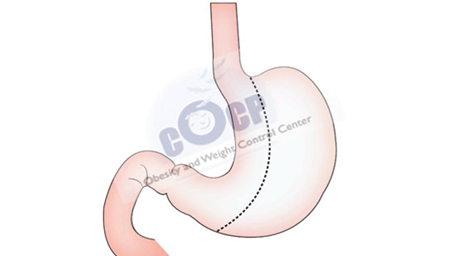
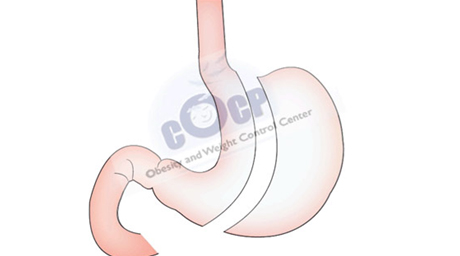
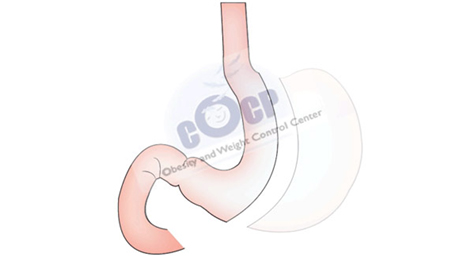
This rising restrictive procedure (<10 years) is based on reducing the size of the stomach, by removing 80-90% of the gastric volume, without any interference with the continuity of the digestive tube. This technique is also called “Calibrated Vertical Gastrectomy” and will give a “banana” shape to the stomach after stapling and removing the fundus of the stomach. Calibration is done over an orogastric tube that is introduced from the mouth into the stomach by the anesthesiologist before performing the stapling.
By removing this reservoir part of the stomach, that has the ability to distend, a feeling of an early satiety is obtained. Another important key to success of this intervention is its hormonal component. The removed gastric part is responsible for the secretion of an important hunger stimulating hormone (Grehlin) which explains the decreased appetite even after small meals. The operative time varies between 45 minutes and 1 hour.

Advantages/Disadvantages
The advantages of Sleeve Gastrectomy are:
The disadvantages of Sleeve Gastrectomy are:
Results
This intervention will achieve 70-100% EWL (Excess Weight Loss) during the first two years and 60-70% EWL in the 5th year on follow-up. The mortality rate of this procedure is very low: 0.05-0.7%.
The morbidity is also quite low with limited early postoperative complications.
It is technically easy, safe and as effective as gastric bypass.
The redo surgery can be a re-sleeve gastrectomy or a plication over the sleeved stomach, a mini gastric bypass, a Roux-en-Y gastric bypass or even more complex surgery such as biliopancreatic diversion and duodenal switch (as a 2nd stage procedure)
Complications
Most patients will not have postoperative complications after Sleeve Gastrectomy, however it can occur. Early complications will depend on the patient’s health status.
These potential risks are not more dramatic than those of any open or laparoscopic procedure (such as appendectomy, hernia repair or gallbladder removal).
One should always keep in mind that the potential risks of obesity surgery are outweighed by its benefits. Thus all kind of possible complication are evoked and explained thoroughly prior to the procedure.
Specific complications for adjustable gastric band are:
Our experience
We have successfully completed more than 506 Sleeve Gastrectomies since 2004. Considered as the pioneers of Laparoscopic Sleeve Gastrectomy in Lebanon, we are performing this procedure almost daily in our institution. The mid-term results are excellent with important excess weight loss in almost all of our series as published in IFSO 2011 (Hamburg), IFSO 2012 (Barcelona) and IFSO 2013 (Istanbul). “What makes our experience and success grow is your trust in us”.